
Bottleneck Opportunity in a New Healthcare Era
An emerging investment theme in clinical research, attractive near-term sector dynamics, and a new stock addition.

Artificial intelligence is actively discovering new drugs.
Both biotech startups and large pharmaceutical companies are seeing returns from AI, which is reducing drug discovery timelines by several multiples compared with traditional approaches.
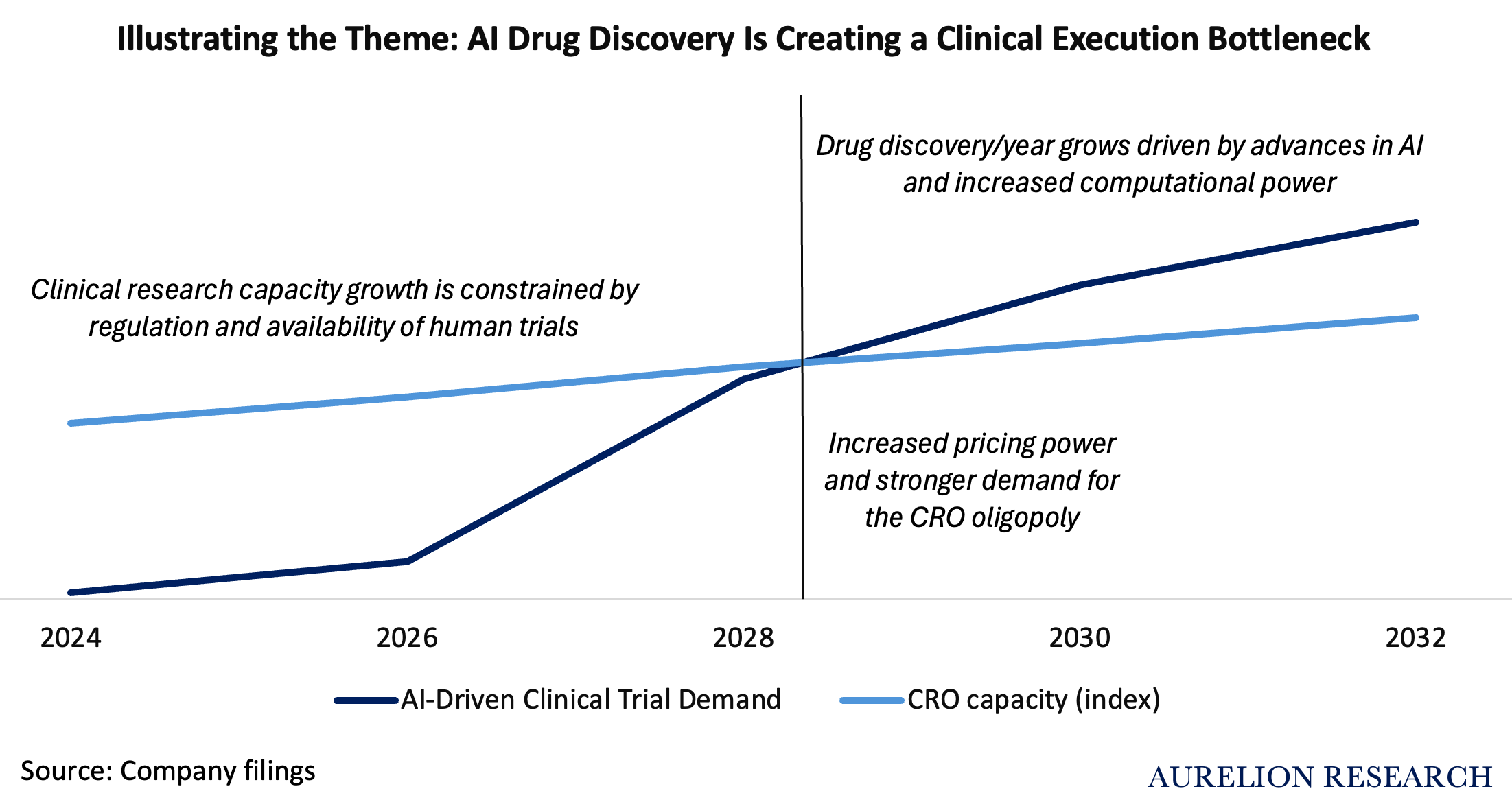
We believe the trend is clear: a surge of new potential drugs will come to the market in the coming years. However, there is a clear bottleneck. Who will run the trials for these drugs?
Contract research organizations (CROs), which benefit from strict FDA regulation and an oligopolistic structure.
This report outlines our investment thesis across three sections:
The Thematic: How the AI-driven surge in drug discovery translates into long-term demand for CROs. And why CROs have been unjustifiably punished.
Industry Dynamics: A dive into the current 2026 landscape, biopharma funding trends, and the operational realities of the CRO oligopoly.
New Aurelion Index stock: The addition of a high-quality differentiated CRO to the portfolio, positioned to benefit from this thematic while currently trading at a cyclical discount.
We avoid gaining exposure to this theme through single biotech names, which carry higher company-specific risk tied to individual drugs.
Three premises are required for the bottleneck to occur:
Premise A: AI increases the volume of preclinical molecular candidates.
Premise B: The FDA requires physical human testing. AI-driven simulations cannot replace biological validation.
Premise C: Clinical trials cannot scale like software. They depend on a finite supply of patients, physicians, and clinics, which makes clinical trials a capacity-constrained process managed by CROs.
Conclusion: The economic bottleneck shifts from drug discovery to clinical trial execution, increasing demand for CROs.
In our view, the most common mistake in thematic investing is timing. Even if the long-term thesis is correct, near-term outcomes are still heavily influenced by industry cycles and CRO operational dynamics. The short to medium term therefore remains critical in this space, and misreading it can lead to poor returns.
For this reason, we also analyze the current 2026 CRO landscape, biotech and biopharma funding trends, and the competitive positioning of key players. We then assess expected returns for leading CROs such as ICON, IQVIA, and CRL.
Table of Contents
Introduction
What is a Contract Research Organization (CRO)
Premise A) Can AI Really Discover Drugs?
Premise B) Regulation and the FDA
Premise C) Physical Limit
The Bottleneck
5.1 The Market’s View
A look at The Bear Case
Recurring Mistake in Thematic Investing: Timing
CRO Industry Overview
8.1 Biotech Funding Trends
8.2 Largepharma Funding Trends
The CRO Market Is Growing
9.1 Biopharma R&D: Where the Growth Is Coming From
9.2 Where Outsourcing Is Growing and Where It Is Not
9.3 Bioprocessing Is Recovering
9.4 Drug Approvals
Diving into Industry Leaders
10.1 ICON ($ICLR)
10.2 Iqvia Holdings ($IQV)
10.3 Charles River Laboratories ($CRL)
10.4 Fortrea Holdings ($FTRE)
New Stock Addition: Best-in Class CRO
11.1 Company Overview
11.2 Why It Is Well Positioned for the Theme
11.3 Competitive Landscape
11.4 Financial Analysis
11.5 Investment Thesis
11.6 Why Now & Recent Developments
11.7 Financial Forecasts and Price Target
11.8 The Bear Case/Risk
11.9 Conclusion
Forecasting Total Return For Major Public CROs